Choice of antihypertensive drug in hypertension
Last reviewed dd mmm yyyy. Last edited dd mmm yyyy
The guidance regarding combination treatment of systemic hypertension has been updated (1):
BP targets in adults:
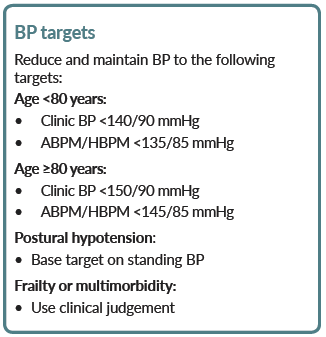
- in people with CKD and diabetes, and also in people with an ACR of 70 mg/mmol or more, aim to keep the systolic blood pressure below 130 mmHg (target range 120-129 mmHg) and the diastolic blood pressure below 80 mmHg
Starting antihypertensive drug treatment
Offer antihypertensive drug treatment in addition to lifestyle advice to adults of any age with persistent stage 2 hypertension. Use clinical judgement for people of any age with frailty or multimorbidity.
Discuss starting antihypertensive drug treatment, in addition to lifestyle advice, with adults aged under 80 with persistent stage 1 hypertension who have 1 or more of the following:
- target organ damage
- established cardiovascular disease
- renal disease
- diabetes
- an estimated 10-year risk of cardiovascular disease of 10% or more
- use clinical judgement for people with frailty or multimorbidity
Consider antihypertensive drug treatment in addition to lifestyle advice for adults aged under 60 with stage 1 hypertension and an estimated 10-year risk below 10%
- note that 10-year cardiovascular risk may underestimate the lifetime probability of developing cardiovascular disease
Consider antihypertensive drug treatment in addition to lifestyle advice for people aged over 80 with a clinic blood pressure of over 150/90 mmHg
- use clinical judgement for people with frailty or multimorbidity
Measure standing as well as seated blood pressure in people with hypertension and:
- with type 2 diabetes or
- with symptoms of postural hypotension or
- aged 80 and over.
- in people with a significant postural drop or symptoms of postural hypotension, treat to a blood pressure target based on standing blood pressure
Offer people with isolated systolic hypertension (systolic blood pressure 160 mmHg or more) the same treatment as people with both raised systolic and diastolic blood pressure
For adults aged under 40 with hypertension, consider seeking specialist evaluation of secondary causes of hypertension and a more detailed assessment of the long-term balance of treatment benefit and risks
Choosing antihypertensive drug treatment
- recommendations in this section apply to people with hypertension with or without type 2 diabetes
- for guidance on choice of hypertensive agent in people with chronic kidney disease, see CKD and hypertension linked item
- people with isolated systolic hypertension (systolic blood pressure 160 mmHg or more) should be offered the same treatment as people with both raised systolic and diastolic blood pressure
- offer antihypertensive drug treatment to women of childbearing potential with diagnosed hypertension in line with guidance below. For women considering pregnancy or who are pregnant or breastfeeding, manage hypertension in line with the recommendations on management of pregnancy
- when choosing antihypertensive drug treatment for adults of black African or African-Caribbean family origin (and not diabetic), consider an angiotensin II receptor blocker (ARB), in preference to an angiotensin-converting enzyme (ACE) inhibitor
Step 1 treatment
Offer an ACE inhibitor or an ARB to adults starting step 1 antihypertensive treatment who:
- have type 2 diabetes and are of any age or family origin or
- are aged under 55 but not of black African or African-Caribbean family origin.
If an ACE inhibitor is not tolerated, for example because of cough, offer an ARB to treat hypertension.
Do not combine an ACE inhibitor with an ARB to treat hypertension
Offer a calcium-channel blocker (CCB) to adults starting step 1 antihypertensive treatment who:
- are aged 55 or over and do not have type 2 diabetes or
- are of black African or African-Caribbean family origin and do not have type 2 diabetes (of any age)
If a CCB is not tolerated, for example because of oedema, offer a thiazide-like diuretic to treat hypertension.
If there is evidence of heart failure, offer a thiazide-like diuretic and follow NICE guidance on management of heart failure
If starting or changing diuretic treatment for hypertension, offer a thiazide-like diuretic, such as indapamide in preference to a conventional thiazide diuretic such as bendroflumethiazide or hydrochlorothiazide
For adults with hypertension already having treatment with bendroflumethiazide or hydrochlorothiazide, who have stable, well-controlled blood pressure, continue with their current treatment
Step 2 treatment
If hypertension is not controlled in adults taking step 1 treatment of an ACE inhibitor or ARB, offer the choice of 1 of the following drugs in addition to step 1 treatment:
- a CCB or
- a thiazide-like diuretic
If hypertension is not controlled in adults taking step 1 treatment of a CCB, offer the choice of 1 of the following drugs in addition to step 1 treatment:
- an ACE inhibitor or
- an ARB
- or a thiazide-like diuretic
If hypertension is not controlled in adults of black African or African-Caribbean family origin who do not have type 2 diabetes taking step 1 treatment, consider an ARB, in preference to an ACE inhibitor, in addition to step 1 treatment
Step 3 treatment
If hypertension is not controlled in adults taking step 2 treatment, offer a combination of:
- an ACE inhibitor or ARB and
- a CCB and
- a thiazide-like diuretic
Step 4 treatment
If hypertension is not controlled in adults taking the optimal tolerated doses of an ACE inhibitor or an ARB plus a CCB and a thiazide-like diuretic, regard them as having resistant hypertension.
Before considering further treatment for a person with resistant hypertension:
- confirm elevated clinic blood pressure measurements using ambulatory or home blood pressure recordings.
- assess for postural hypotension.
- discuss adherence
For people with confirmed resistant hypertension, consider adding a fourth antihypertensive drug as step 4 treatment or seeking specialist advice
Consider further diuretic therapy with low-dose spironolactone for adults with resistant hypertension starting step 4 treatment who have a blood potassium level of 4.5 mmol/l or less. Use particular caution in people with a reduced estimated glomerular filtration rate because they have an increased risk of hyperkalaemia
When using further diuretic therapy for step 4 treatment of resistant hypertension, monitor blood sodium and potassium and renal function within 1month of starting treatment and repeat as needed thereafter
Consider an alpha-blocker or beta-blocker for adults with resistant hypertension starting step 4 treatment who have a blood potassium level of more than 4.5mmol/l.
If blood pressure remains uncontrolled in people with resistant hypertension taking the optimal tolerated doses of 4 drugs, seek specialist advice
Notes:
Stage 1 hypertension
- clinic blood pressure ranging from 140/90 mmHg to 159/99 mmHg and subsequent ABPM daytime average or HBPM average blood pressure ranging from 135/85 mmHg to 149/94 mmHg
Stage 2 hypertension
- clinic blood pressure of 160/100 mmHg or higher but less than 180/120 mmHg and subsequent ABPM daytime average or HBPM average blood pressure of 150/95 mmHg or higher
Stage 3 or severe hypertension
- clinic systolic blood pressure of 180 mmHg or higher or clinic diastolic blood pressure of 120 mmHg or higher.
Reference:
Related pages
- Elderly hypertensives
- Combination ACD drug therapy in hypertension
- Aspirin in hypertensive patients
- Cholesterol and hypertension
- Beta-blockers in hypertension
- Thiazides in hypertension
- Calcium antagonist in hypertension
- ACE inhibitors in hypertension
- Angiotensin II receptor inhibitors in hypertension
- Selective imidazoline receptor antagonists
- Systemic hypertension
- Withdrawal of antihypertensive medication
- Renin inhibitors in hypertension
- Oral hypertensive treatments
- Hypertension in chronic kidney disease (CKD)
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.