Shoulder Injury Related to Vaccine Administration (SIRVA)
Shoulder Injury Related to Vaccine Administration (SIRVA)
What's the Problem?
The deltoid muscle is the ideal site for achieving excellent immunity when giving vaccine injections.
Naturally a degree of local inflammation with some discomfort, is to be expected.
But even in experienced hands, jabs are not without risk, and if the injectate reaches unintended places, it can produce a vigorous immune response where it is not wanted, especially in pre-primed individuals.
There are 3 types of unwanted local reactions (1):
- Cutaneous / subcutaneous... the commonest
- Nerve injuries...fortunately rare
- Shoulder joint mechanism problems...? under-recognised
Cutaneous / subcutaneous reactions
These are more likely to occur when the injection fails to reach muscle, or gets infected.
Changes include:
- localised fat loss
- local inflammation with nodule or abscess formation
- cellulitis
- (very rarely, necrosis from vascular complications).
Most of the problems are minor in nature.
Nerve injuries
Direct needle injury, or damage to accompanying vessels with bleeding and local pressure, will usually rapidly become apparent.
A local inflammatory response takes longer to develop, but is far less likely with the small volume vaccine injections than in cases following deltoid injections with therapeutic substances, which may also have neurotoxic effects. (Therapeutic injections are not often used at this site in the West).
Two nerves are at risk of palsy:
- the Radial (most commonly affected), and the Axillary
- both pass deep to the deltoid
Shoulder joint mechanism problems, aka SIRVA
All parts of the shoulder joint apparatus have been adversely affected, from the bursa under the deltoid, down to the underlying bone itself, notably presenting as:
- Bursitis
- Frozen Shoulder (Periarthritis)
- Rotator Cuf Syndrome (affecting one or more tendons)
In 2010 the term "SIRVA" (Shoulder Injury Related to Vaccine Administration) was coined in the United States to describe the spectrum of conditions resulting in... "shoulder pain with limited range of movement within 48 hours after vaccination receipt in individuals with no prior history of pain, inflammation or dysfunction of the affected shoulder before vaccine administration".
An in-depth study of VAERS (Vaccine Associated Event Reporting System) following flu jabs, concluded that such shoulder problems still present at 7 days post-jab, lasted on average 70 days (range 18-365 days), and probably accounted for 2% of all adverse event reports. (2)
By 2020, over half the claims for compensation post-vaccination in the States, were for this.
In the UK, there is not yet equivalent research, and the issue is not easy to annalyse.
Being a medico-legal term, there is no SNOMED code, but it is listed in the Yellow Card System for expected reactions.
Even with the restrictions resulting from the Pandemic, checking the System for "SIRVA" and the three terms listed above, revealed 1617 reports following COVID 19 immunisations, by May 2022. (3)
Unusual then, but not insignificant for the affected individuals.
And avoidable....
Where to inject, then ?
Half way down the deltoid muscle is the accepted wisdom, where it is usually thick.
But some simplified training diagrams may not explain the muscle properly, as here. [Fig 1]:
Fig 1 - Training programmes tend to use simplified diagrams that can be misleading, like this
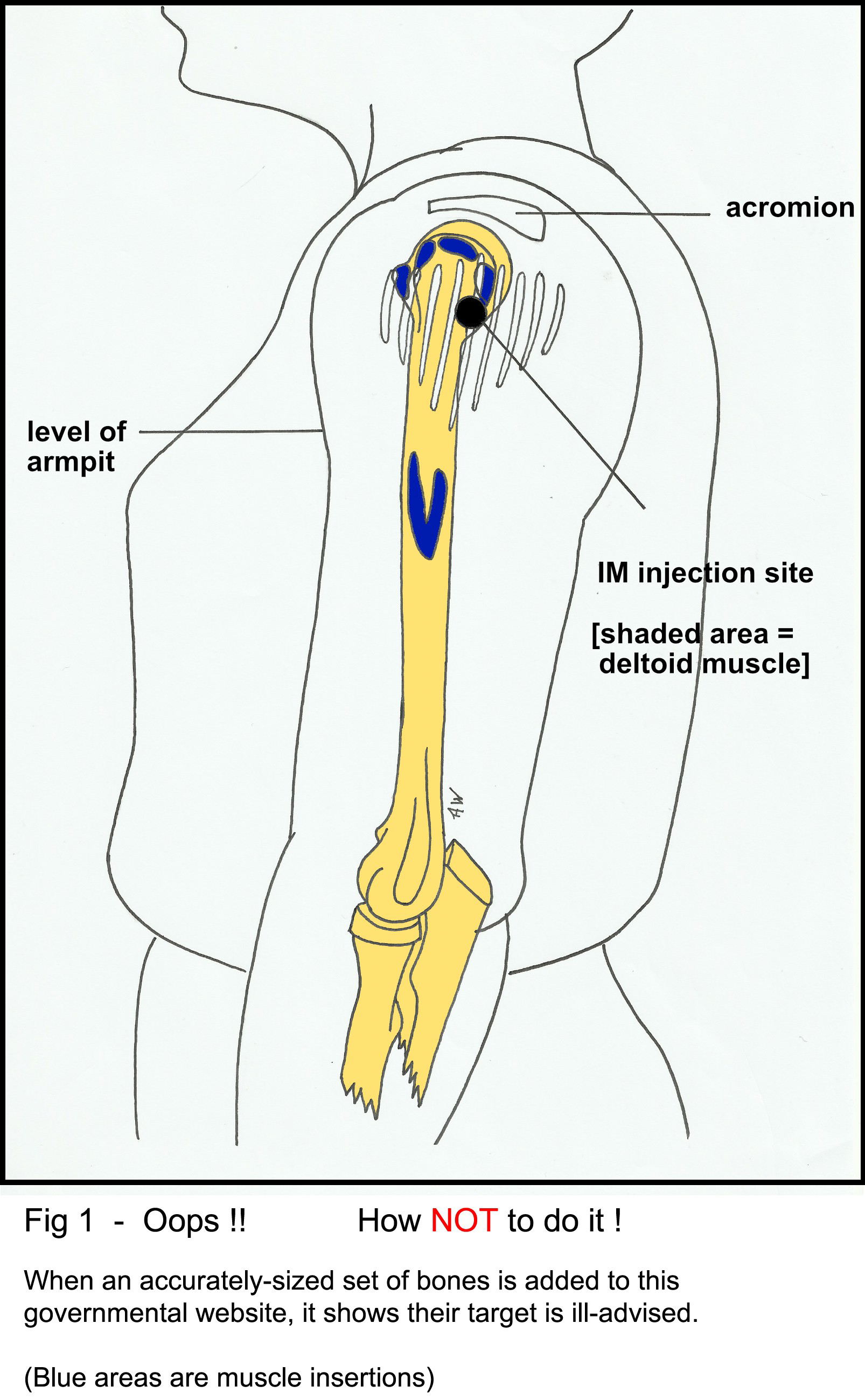
The deltoid is triangular with its point downwards.
- The target [central] section runs vertically down from the acromion.
- The tip of the muscle is halfway down the humerus.
- The V-shaped insertion [4-5 cm long], gets more fibrous below the axillary skin folds, and is usually avoided.
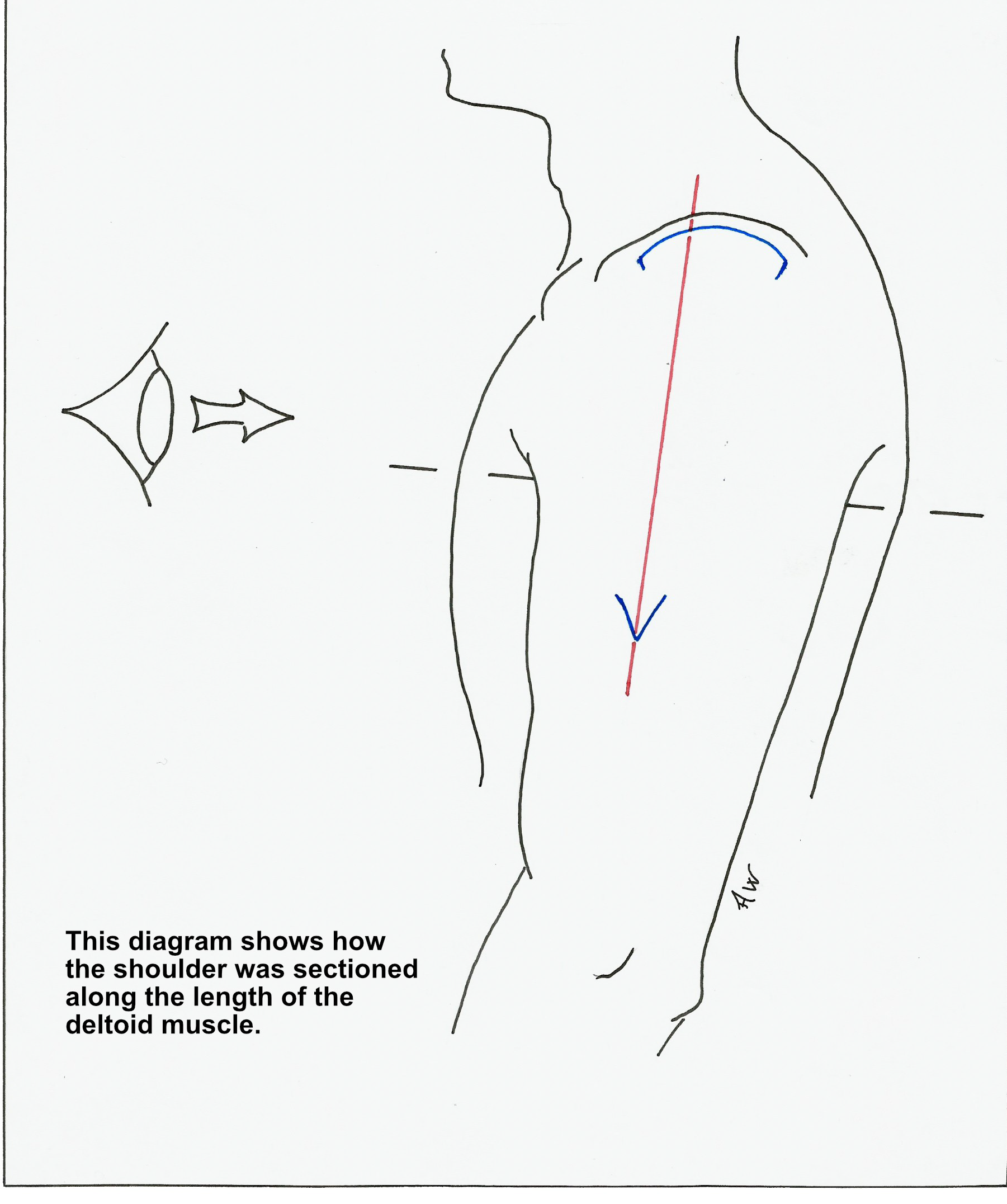
Fig 2 - Explains the following views of a cut shoulder (Fig 3, Fig 4 and Fig 5)
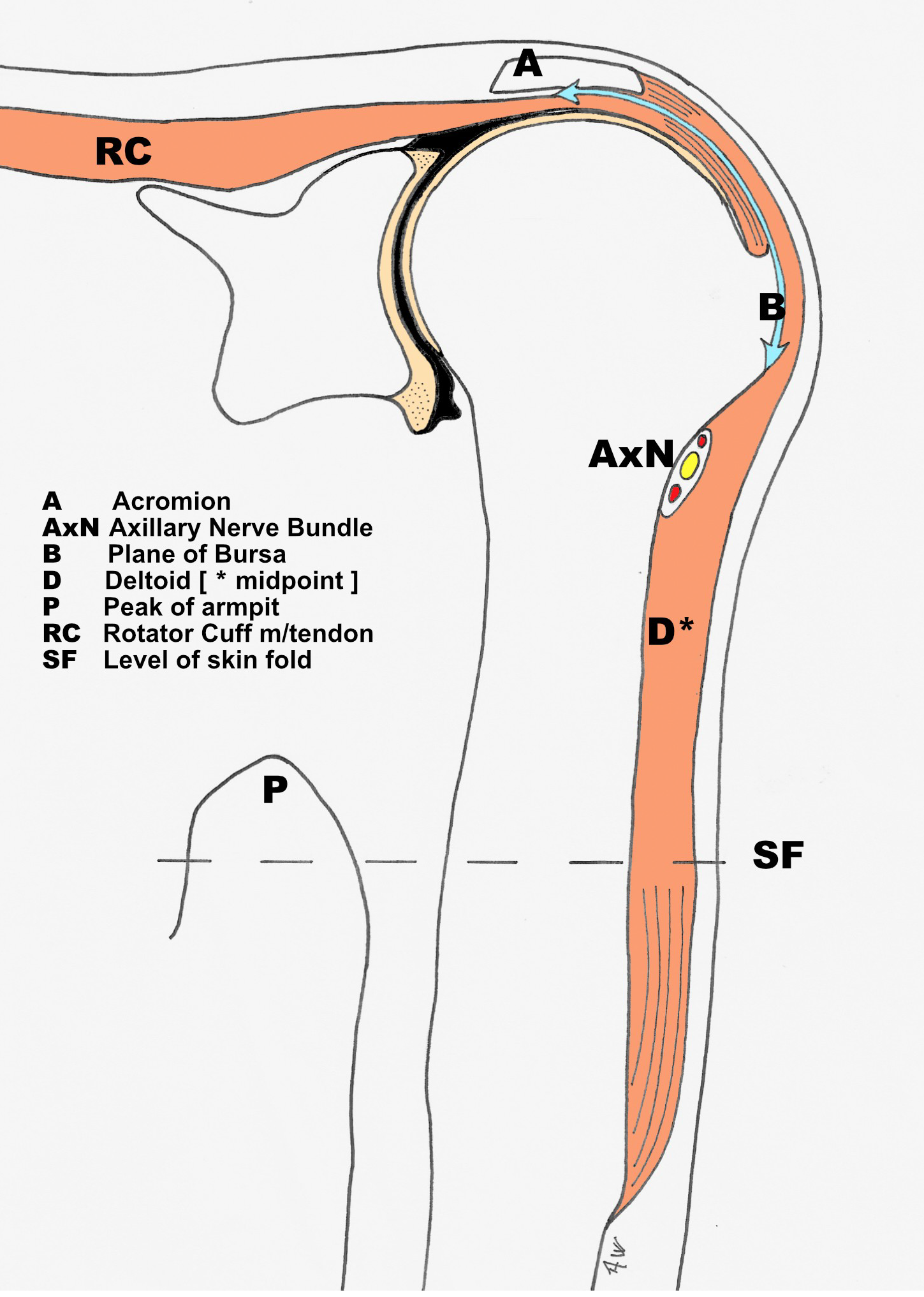
At Risk Structures
- Directly under the upper third of the deltoid are:
- The compressible and highly mobile bursa [which doesn’t extend beyond the axillary nerve.
- The joint capsule.
- The rotator cuff muscles/tendons.
- The articular cartilage and bone.
- Further down:
- The axillary nerve and accompanying blood vessels.
- When measured below the acromial edge by ultrasound of the skin surface, these can lie as far as 9.2 cm in the adult male, and 7.7 in the adult female (4).
- Radial Nerve:
- This nerve and its vessels pass downwards behind the posterior part of the deltoid, spiralling round the humerus alongside its insertion..avoid this part ! (5)
Fig 3 Vertical section through midline of deltoid
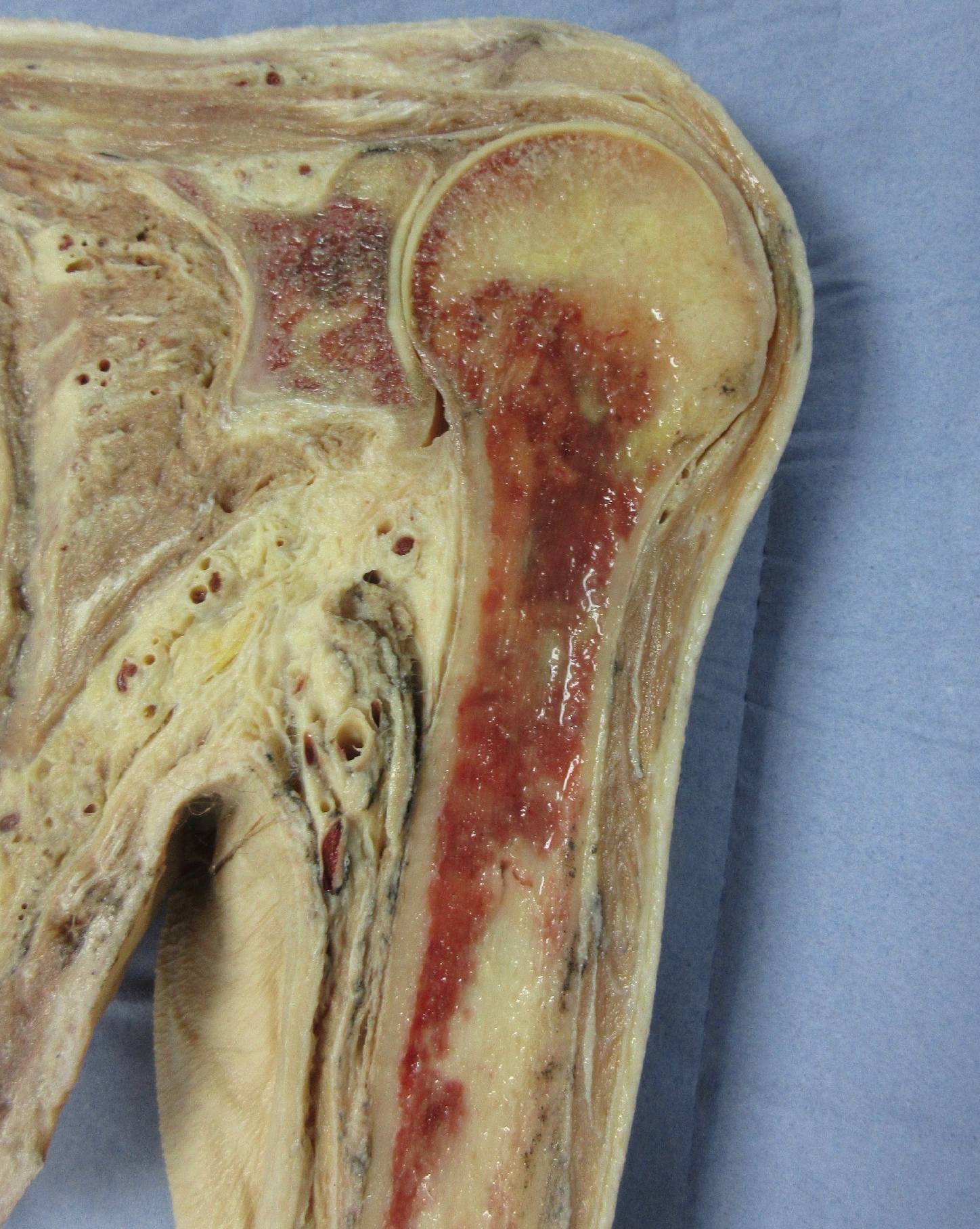
Key to photograph
Handy Protection Guide!
- The patient's opposite hand can serve as a guide.
- Swing across and align so the top of the index lies along the lower edge of the acromion.
- This covers the vulnerable structures [Figs 4, 6] (5)
- This must be the patient's OWN hand, NOT the vaccinator's, which may not be in proportion.
- The target zone remains in a line vertically below the midpoint of the acromion. [Fig 6]
- Other positions; arm resting on desk, hand on hip, etc, alter the anatomy under the skin.
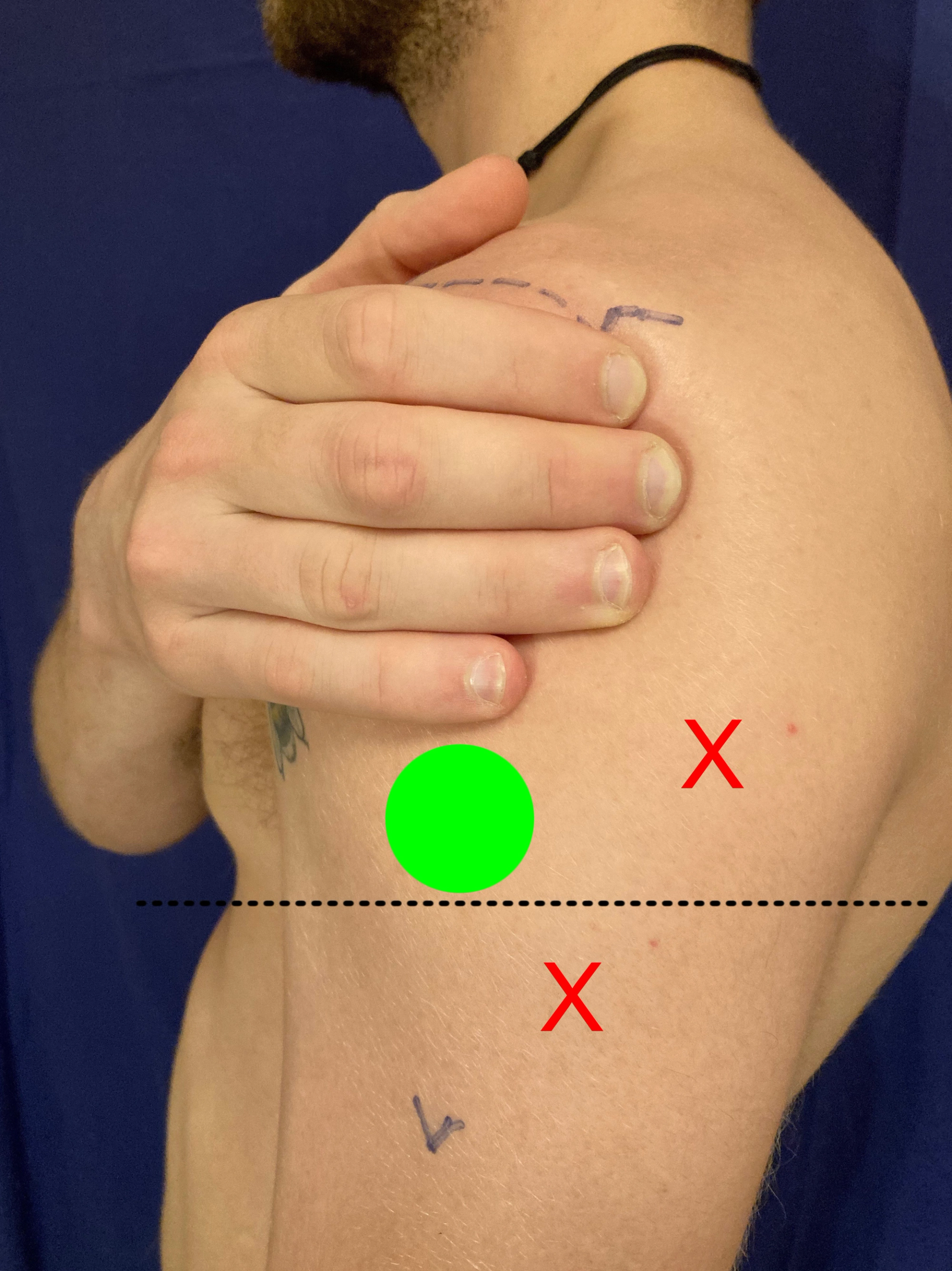
Fig 4 - "Target Zone" (green)

- NB It should be the patient’s own hand and NOT the vaccinator’s, as these may not be in proportion
Needles
- Most vaccines need to be injected into muscle.
- A 25mm needle will reach muscle in adults of average build. (6)
- Deposition in subcutaneous fat is more likely to suffer a reaction, so in large individuals, longer is recommended…
- Adult males over 118kg [18st 8lb], and females over 90kg [14st 2lb] require 38mm.
- With small subjects or slim build, 25mm needles may reach bone, so caution and judgement are required. [Fig 5]
- American guidelines still mention the 16mm option for adults females below 60kg [9st 6lb]. (7)
- The risk of over-penetration in childrens’ arms, is high. (8)
Fig 5 Needle depth should be to suit the individual
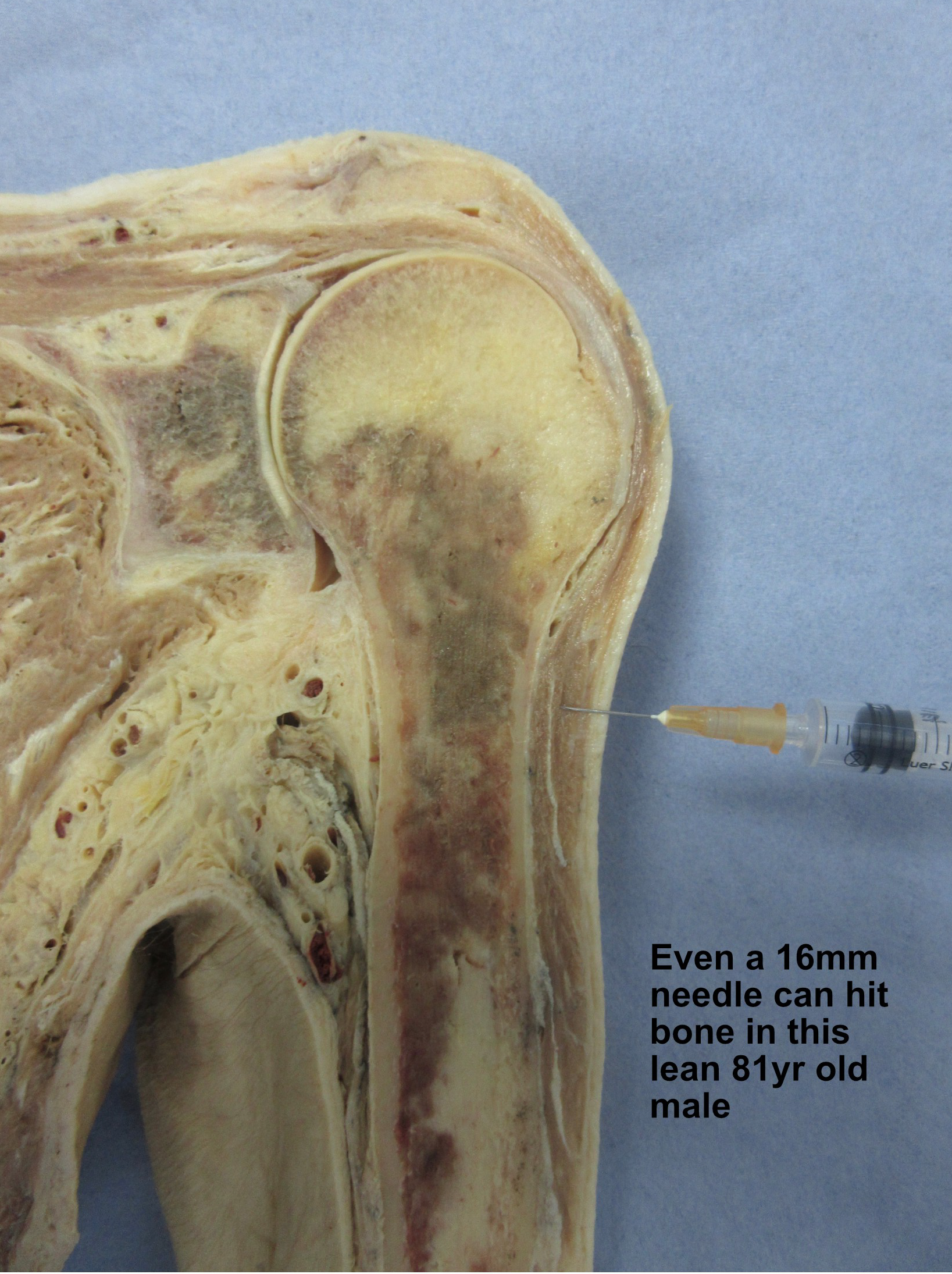
Fig 6 - Target area (in green) X = Avoid the posterior part of the muscle
- Summary
- sit the patient
- let the arm hang loosely down at the side, with the hand in its relaxed, neutral position
- place the patient's own hand, with the top of the index along the lower border of the acromion
- inject in the mid-line, between the little finger and the level of the armpit skinfolds, (a 2-3cm target in adults)
- get on a level to check, and inject at 90 degrees to the skin surface
- use a 25mm needle for adults of average build; longer for large individuals; shorter for slim or small subjects
- Key Learning Points:
- the mid-point of the deltoid is usually recommended for vaccinations; structures above this level do get damaged
- you will get the mid-point wrong if you don’t know the full extent of the muscle
- moving the arm arm into different positions [resting it on a desk, placing the hand on the hip, +c], alters the anatomy under the skin
- think about the needle length for each patient
- and most importantly:
- it is safer to aim a fraction below the midpoint, than to go above it
Remember!
- You will get the deltoid's mid-point WRONG if you don’t know its full extent.
- It's safer to go a fraction below the mid-point, than above.
Contributor:
- Alan Walker Retired GP , and Ex-Anatomy Lecturer; Affiliated to Hull York Medical School, and the Primary Care Rheumatology and Musculoskeletal Society
Acknowledgements:
- Cadaveric imaging taken with appropriate donor consent from Hull York Medical School. Especial thanks to the donor and their family; to HYMS colleagues, Rachel Cunningham and Martin Walters, for their assistance; to those who added constructive criticism; and to my family, as always.
Reference:
- Cook IF. Best vaccination practice and medically attended injection site events following deltoid intramuscular injection. Hum Vaccin Immunother. 2015; 11[5]1184-1191 htpps//doi.org/10.1080/21645515.2015.1017694
- Hibbs BF et al. Reports of atypical shoulder pain and dysfunction following inactivated influenza vaccine, Vaccine Adverse Event Reporting System [VAERS], 2010-2017 Vaccine. 2020; 38:1137-1143 htpps//doi.org/10.1016/j.vaccine.2019.11.023
- MHRA Coronavirus vaccines adverse reactions. Yellow Card Reports up to 11/5/2022
- Nakajima Y, Mukai K, Takaoka K, et al. Establishing a new appropriate intramuscular injection site in the deltoid muscle. Hum Vaccin Immunother. 2017; 13: 2123-2129 https://doi.org/10.1080/21645515.2017.1334747
- Walker A, You know where you can stick that !!…or do you ? Where to inject the deltoid, and why. Practice Nursing. 2021; 32 [5]; 189-193 magonlinelibrary.com/doi/full/10.12968/pnur.2021.32.5.189
- Poland GA, Borrud A, Jacobson RM, et al. Determination of deltoid fat pad thickness. Implications for needle length in adult immunization.
JAMA. 1997; 277 [221]: 1709-1711 https://doi.org/10.1001/jama.277.21.1709 - The Pink Book: Epidemiology of Vaccine-Preventable Diseases. Centers for Disease Control and Prevention, USA, 2021
- Lippert WC, Wall EJ. Optimal Intramuscular Needle Penetration Depth. Pediatrics. 2008; 122 [3]: e556-e563. https://doi.org/10.1542/peds.2008-0374
Related pages
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.