Compression bandaging
Provided that arterial disease has been excluded, the treatment of choice in venous ulceration is compression bandaging combined with exercise. Bandaging works by providing active counterpressure to the hypertensive venous blood and by improving the function of the muscle pump.
A suitable compression system should:
- be capable of providing graduated compression from ankle to knee
- be capable of sustaining the pressure for 7 days
- provide reproducible, safe compression
- be comfortable for the patient and allow them to wear outdoor shoes
- be accepted by the patient
Before applying the bandage, measure the person's ankle circumference and apply below-knee, graduated multi-layer high compression bandaging and replace weekly (1).
General advice (2):
Do not routinely include ’made to measure’ on the prescription. ‘Made to measure’ should only be selected if the patient has had their leg measurements checked in the past six months and none of the standard sizes are appropriate. If in doubt discuss with the community pharmacist or community nurse.
- to avoid confusion hosiery can be prescribed as generic e.g. ‘compression hosiery class 1 below knee
- compression hosiery is palliative not curative and treatment should continue for as long as there is evidence of venous disease – in most cases this is life-long (exc. pregnancy)
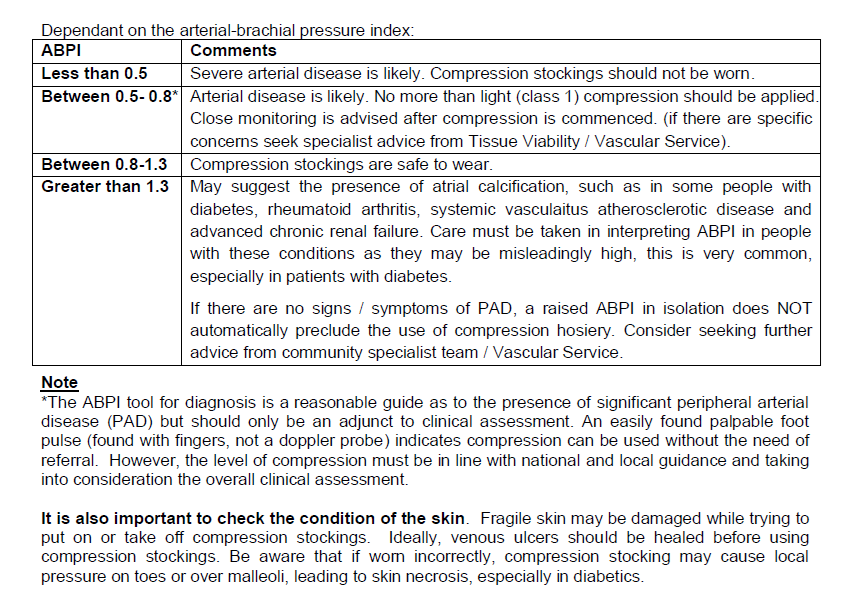
- compression hosiery should not be applied if there is a history or presentation of symptomatic peripheral arterial disease (PAD) (see assessment criteria)
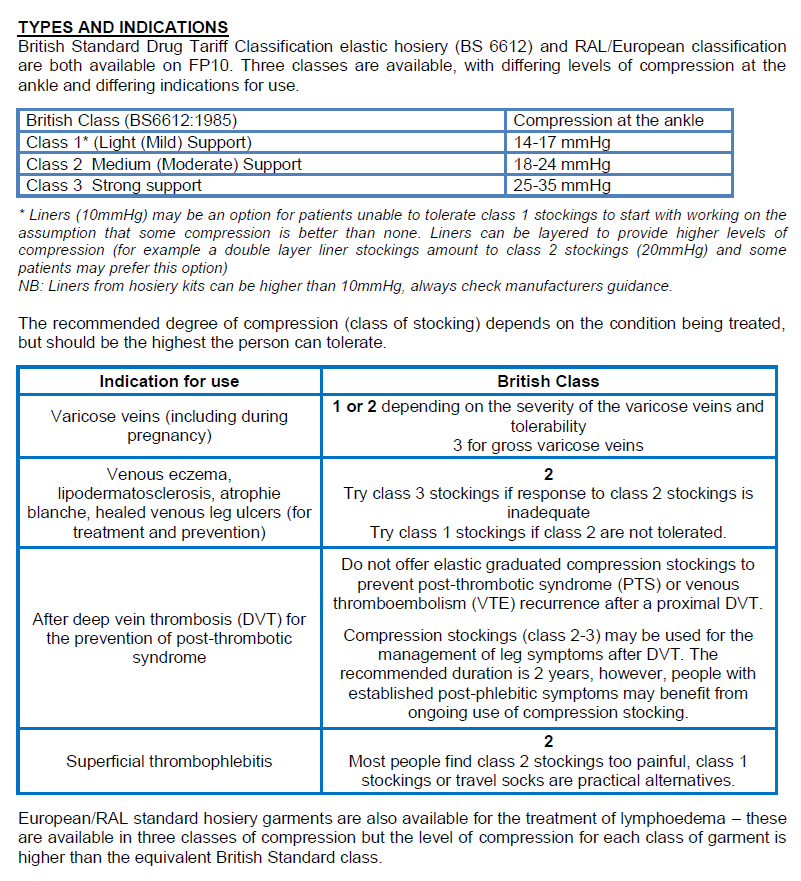
- in the absence of any of the risk factors in the assessment criteria it is safe to start with compression hosiery up to 20mmHg, which is defined as mild graduated compression
- the Ankle Brachial Pressure Index (ABPI) test should be used as guide to assess the presence of significant PAD but should only be an adjunct to clinical assessment
- for patients requiring higher than 20mmHg compression hosiery e.g. to treat moderate/severe oedema, ABPI is required. Consider the use of a milder compression whilst waiting for the Doppler assessment to avoid deterioration of condition if appropriate and dependant on the results of a thorough assessment. An ABPI is also recommended if starting with Class 3 support stockings
- all patients with chronic venous leg ulcers should have a lower limb assessment performed prior to treatment
- arterial insufficiency should be investigated further by the vascular team to ensure adequate circulation if clinically appropriate
- the recommended degree of compression depends on the condition being treated. If the person cannot tolerate the preferred compression for their condition, try the next level down
- ideally, lower limb assessments should be repeated every 6–12 months or earlier if clinically indicated
- patients treated with compression hosiery should be reviewed every 6 months (with repeat lower limb assessment if appropriate) to reassess the condition for disease deterioration and to ensure the person is continuing to wear the stocking correctly and successfully
- compression hosiery for the sole prevention of deep vein thrombosis (DVT) for travellers is not available on NHS prescription and patients should be advised to purchase class 1 below knee stockings or proprietary “flight socks”.
Assessment (2):
Compression hosiery should not be applied if there is a history or presentation of symptomatic peripheral arterial disease (PAD). Before prescribing, the patient should be assessed for the following:
- acute infection of the leg/foot (increasing unilateral redness, swelling, pain, heat)
- symptoms of sepsis
- acute or chronic limb-threatening ischaemia
- suspected acute DVT
- suspected skin cancer
- painful cramping in calf muscles during activity e.g.walking or climbing stairs (intermittent claudication)
- leg numbness or weakness
- cold leg and/or foot, especially when compared with the other side
- absent or difficult to feel foot pulse
- poor capillary refill (should be less than 2 seconds)
- drop in pulse oximetry on leg elevation
- if any one or more of these is present, arterial insufficiency should be excluded by measuring the ABPI using a Doppler machine, performed by a suitably trained and competent healthcare professional
- all patients with chronic venous leg ulcers should have a lower limb assessment performed prior to treatment which may include an ABPI using a Doppler ultrasound
Reference:
- NICE 2008. Leg ulcer-venous
- Derbyshire Joint Area Prescribing Committee. Guidelines for the use of compression hosiery (accessed 14th July 2024).
Related pages
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.