Diagnosis of asthma in adults and children
The diagnostic process for asthma varies with respect to the age of the individual who has possible asthma:
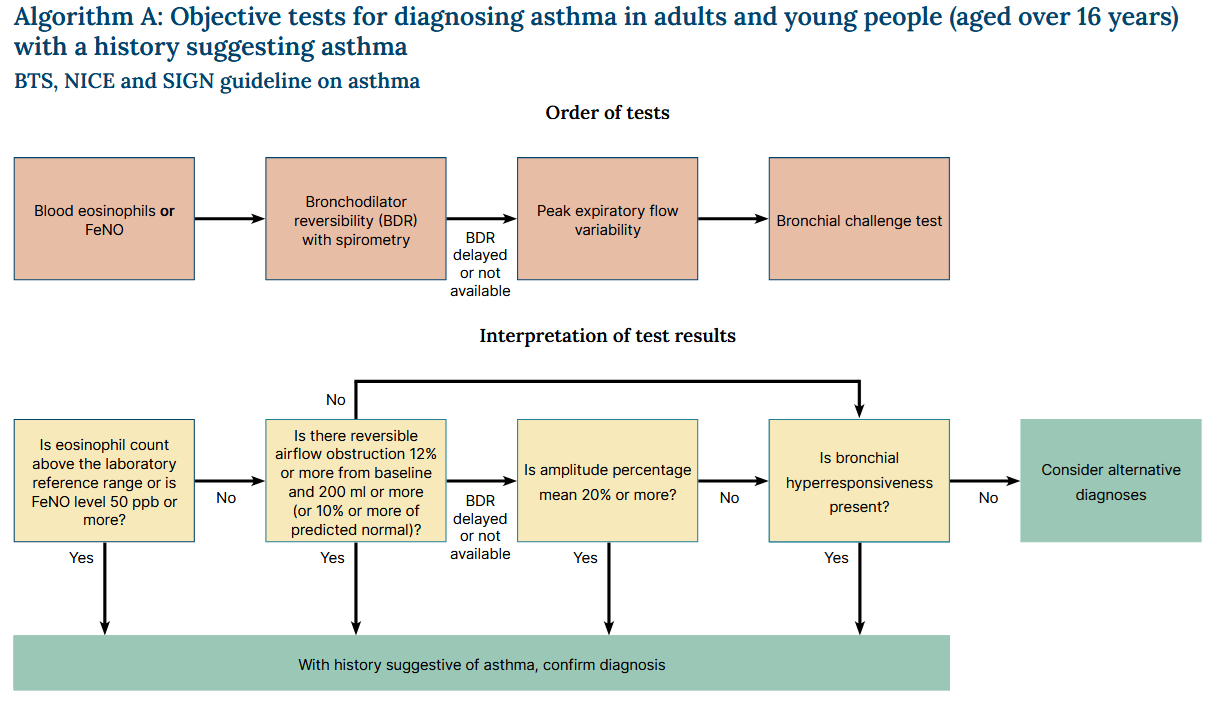
Diagnosing asthma in individuals aged 16 and over
The process of diagnosis in individuals aged 16 and over is summarised:
Detailed commentary:
- in adults with a history suggestive of asthma, measure the blood eosinophil count or fractional exhaled nitric oxide (FeNO) level
- asthma is diagnosed if the eosinophil count is above the laboratory reference range or the FeNO level is 50 ppb or more
- measure bronchodilator reversibility (BDR) with spirometry if asthma is not confirmed by eosinophil count or FeNO level
- diagnose asthma if the FEV1 increase is 12% or more and 200 ml or more from the pre-bronchodilator measurement (or if the FEV1 increase is 10% or more of the predicted normal FEV1)
- if spirometry is not available or it is delayed, measure peak expiratory flow (PEF) twice daily for 2 weeks.
- diagnose asthma if PEF variability (expressed as amplitude percentage mean) is 20% or more
- if asthma is not confirmed by eosinophil count, FeNO, BDR or PEF variability but still suspected on clinical grounds, refer for consideration of a bronchial challenge test
- diagnose asthma if bronchial hyper-responsiveness is present
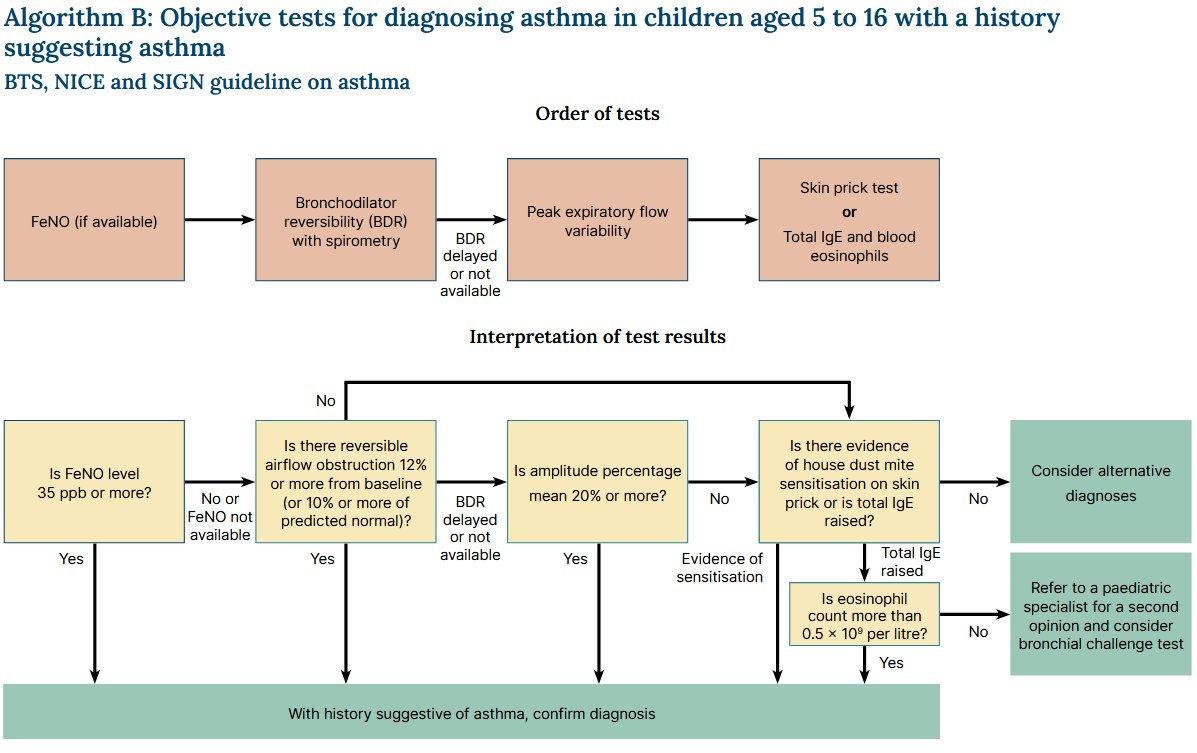
Diagnosing asthma in individuals aged 5 to 16 years old
The process of diagnosis of asthma in children aged 5 to 16 years old is summarised:
Detailed commentary:
- in children with a history suggestive of asthma then measure the FeNO level
- diagnose asthma if the FeNO level is 35 ppb or more
- measure BDR with spirometry if the FeNO level is not raised, or if FeNO testing is not available
- diagnose asthma if the FEV1 increase is 12% or more from baseline (or if the FEV1 increase is 10% or more of the predicted normal FEV1)
- if spirometry is not available or it is delayed, measure PEF twice daily for 2 weeks
- diagnose asthma if PEF variability (expressed as amplitude percentage mean) is 20% or more
- if asthma is not confirmed by FeNO, BDR or PEF variability but still suspected on clinical grounds, either perform skin prick testing to house dust mite or measure total IgE level and blood eosinophil count
- exclude asthma if there is no evidence of sensitisation to house dust mite on skin prick testing or if the total serum IgE is not raised
- diagnose asthma if there is evidence of sensitisation or a raised total IgE level and the eosinophil count is more than 0.5 x 109 per litre
If there is still doubt about the diagnosis, refer to a paediatric specialist for a second opinion, including consideration of a bronchial challenge test.
Diagnosing asthma in children under 5
Diagnosis is hard in this age group because it is difficult to do the tests and there are no good reference standards:
- for children under 5 with suspected asthma, treat with inhaled corticosteroids in line with the recommendations on medicines for initial management in children under 5 and review the child on a regular basis
- if they still have symptoms when they reach 5 years, attempt objective tests
- if a child is unable to perform objective tests when they are aged 5:
- attempt to do the tests again every 6 to 12 months until satisfactory results are obtained
- refer for specialist assessment if the child's asthma is not responding to treatment
Reference:
Related pages
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.