Rotator cuff tear
The rotator cuff is the sheath of conjoint tendons which run over the top of the shoulder capsule and inserts into the greater tuberosity of the humerus
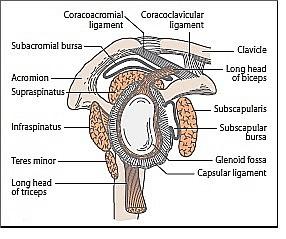
- the tendons are those of the short muscles of the shoulder - supraspinatus, infraspinatus, teres minor and subscapularis
- the cuff is covered anteriorly by the coracoacromial arch with the subacromial bursa in between
- the main role of the cuff is to stabilise the humeral head within the glenoid, particularly when the arm is flexed or abducted by the deltoid muscle
Muscle | Origin on scapula | Attachment on humerus | Function | Innervation |
subscapularis muscle | subscapular fossa | lesser tuberosity (60%) or humeral neck (40%) | internally rotates the humerus | subscapular nerve (C5-6) |
supraspinatus muscle | supraspinous fossa | inserts on the middle facet of the greater tuberosity | abduction of the arm | suprascapular nerve (C5) |
infraspinatus muscle | infraspinous fossa | inserts posterior facet of theon the greater tuberosity | externally rotates the arm | suprascapular nerve (C5-6) |
teres minor muscle | middle half of the lateral border | inserts on the inferior facet of the greater tuberosity | externally rotates the arm | axillary nerve (C5) |
The subacromial space lies underneath the acromion, the coracoid process, the acromioclavicular joint and the coracoacromial ligament. A bursa in the subacromial space provides lubrication for the rotator cuff
Supraspinatus is the cuff tendon most liable to injury. It is the most exposed of the tendons - running over the top of the shoulder under the anterior edge of the acromion and the adjacent acromioclavicular joint - and also has a relatively poor arterial blood supply near to it's insertion into the greater tuberosity. Consequently, `supraspinatus' is often used synonymously with `rotator cuff' when describing lesions of this area.
- the rotator cuff is the dynamic stabilizer of the glenohumeral joint
- the static stabilizers are the capsule and the labrum complex, including the glenohumeral ligaments
- although the rotator cuff muscles generate torque, they also depress the humeral head
- the deltoid abducts the shoulder
- without an intact rotator cuff, particularly during the first 60 degrees of humeral elevation, the unopposed deltoid would cause cephalad migration of the humeral head, with resulting subacromial impingement of the rotator cuff
- in patients with large rotator cuff tears, the humeral head is poorly depressed and can migrate cephalad during active elevation of the arm. This migration is sometimes evident even on plain radiographs
- the space between the undersurface of the acromion and the superior aspect of the humeral head is called the impingement interval
- this space is normally narrow and is maximally narrow when the arm is abducted. Any condition that further narrows this space can cause impingement
Notes:
- rotator cuff impingement syndrome
- rotator cuff muscle tendons pass through a narrow space between the acromion process of the scapula and the head of the humerus
- symptoms include pain, weakness and loss of motion
- anything which causes further narrowing of this space can result in impingement syndrome
- causes include
- bony structures such as subacromial spurs (bony projections from the acromion), osteoarthritic spurs on the acromioclavicular joint, and variations in the shape of the acromion
- thickening or calcification of the coracoacromial ligament
- loss of function of the rotator cuff muscles, due to injury or loss of strength, may cause the humerus to move superiorly, and cause impingement
- inflammation and subsequent thickening of the subacromial bursa
- however within the rotator cuff, supraspinatus is the cuff tendon most liable to injury. It is the most exposed of the tendons - running over the top of the shoulder under the anterior edge of the acromion and the adjacent acromioclavicular joint - and also has a relatively poor arterial blood supply near to it's insertion into the greater tuberosity. Consequently, `supraspinatus' is often used synonymously with `rotator cuff' when describing lesions of this area
- causes include
- clinical features
- pain, weakness and loss of motion are the most common symptoms reported
- pain is exacerbated by overhead or above-the-shoulder activities
- a frequent complaint is night pain, often disturbing sleep, particularly when the patient lies on the affected shoulder
- onset of symptoms may be acute, following an injury, or insidious, particularly in older patients, where no specific injury occurs
- there may be a grinding or popping sensation during movement of the shoulder
- range of movement may be limited by pain
- a painful arc of movement may be present during forward elevation of the arm from 60° to 120°
- passive movement at the shoulder will appear painful when a downwards force is applied at the acromion but the pain will ease once the downwards force is removed
- pain, weakness and loss of motion are the most common symptoms reported
- click here for a video of examination of the rotator cuff
- rotator cuff muscle tendons pass through a narrow space between the acromion process of the scapula and the head of the humerus
Reference
- Weber S, Chahal J. Management of rotator cuff injuries. J Am Acad Orthop Surg. 2020 Mar 1;28(5):e193-201.
- Expert Panel on Musculoskeletal Imaging; Amini B, Beckmann NM, Beamanet FD, al. ACR appropriateness criteria: shoulder pain - traumatic. J Am Coll Radiol. 2018 May;15(5s):S171-88.
Related pages
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.