Doses are of oestrogen in oral preparations are an order of magnitude greater than the transdermal route. This is because oral preparations are absorbed through the gut and of into the hepatic portal circulation where most of the oestrogen is removed by first-pass metabolism.
There are a number of different preparations available. These include:
- oestrogen only - used post hysterectomy:
- conjugated equine oestrogens (CEE) e.g. Premarin
- oestradiol valerate (E2V) e.g. Progynova
- piperazine oestrone sulphate e.g. Harmogen
- opposed oestrogen - 28 day cycles:
- CEE days 1-28; norgestrel days 17-28 e.g. Elleste Duet 1mg or 2mg
- E2V days 1-28; norgestrel days 17-28 e.g. Nuvelle
- E2/E3 days 1-28; norethisterone days 19-28 e.g. Trisequens
Continuous combined oestrogen progestogen therapy: this is suitable for women suffering from menopausal symptoms a year or more after the menopause; this form of HRT is particularly suitable for those women who are intolerant of progestogens and dislike the idea of a withdrawal bleed. Therapies available in the UK include:
- Premique low dose
- Kliofem (norethisterone 1mg plus oestradiol valerate 2mg)
- Kliovance
- Climesse
Breakthrough bleeding is a common problem with combined preparations and occurs in 25-30% of patients in the first 3-6 months of use of a continuous combined preparation (1).
A suggested algorithm for use of HRT is presented (2):
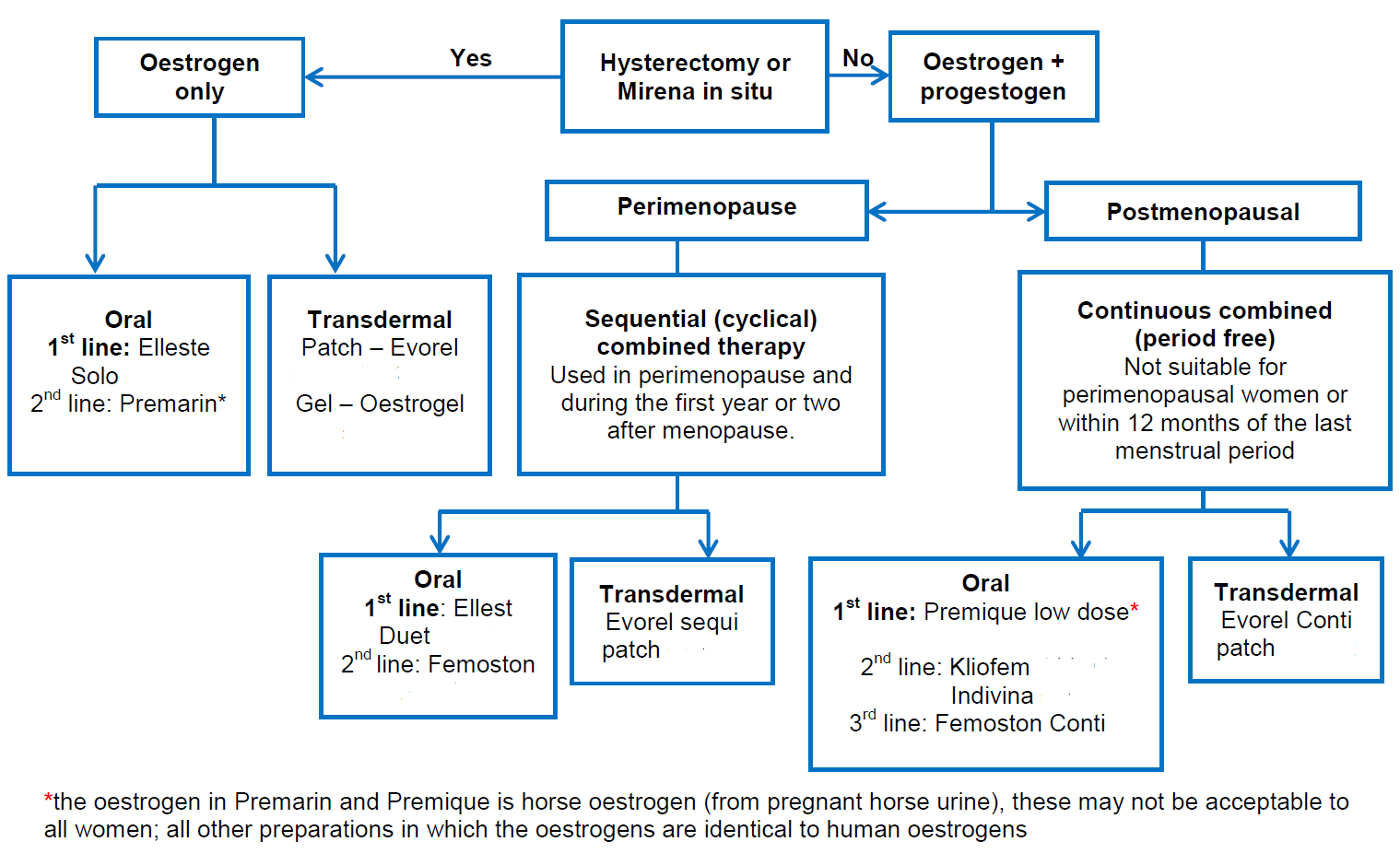
Notes (2):
- choice of HRT
- choice of HRT for an individual depends on an overall balance of indication, risk-benefit profile, side effects and convenience. Prescribe the lowest effective dose of HRT for the shortest time possible.

- Risks associated with HRT (1)
- HRT does not increase cardiovascular (CVS) risk when started under age 60
- HRT is not contraindicated in women with optimally managed CVS risk factors (eg hypertension, diabetes)
- consider transdermal HRT in women with a higher background VTE risk including those with a BMI over 30 kg/m2 as oral HRT is associated with a higher risk of venous thromboembolism.
- HRT with oestrogen (ET) alone is associated with little or no change in the risk of breast cancer, combined oestrogen and progestogen HRT (CET) can be associated with an increase in the risk of breast cancer: however the latter is required in women with a uterus
- Patches versus oral preparations
- patches are more expensive than oral preparations but may be suitable for patients with high risk of VTE (e.g. those with a BMI over 30 kg/m2) - consider referring those at high risk (strong family history of VTE or a hereditary thrombophilia) to a haematologist for assessment before considering HRT
- transdermal routes avoid the first pass effect through the liver and are not associated with increased low density lipoproteins, venous thrombosis or stroke. Patches deliver a more steady level of hormone which can be helpful in conditions triggered by fluctuating levels eg migraine.
Reference:
- (1) Hickey M, Elliott J, Davison SL.Hormone replacement therapy. BMJ. 2012;344:e763.
- (2) Derbyshire Joint Prescribing Committee. Menopause Management Guideline (Accessed 13th March 2019)
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.