Measles is a clinical diagnosis. (although in UK this has a low positive predictive value since the incidence of measles is low) (1)
In Summary:
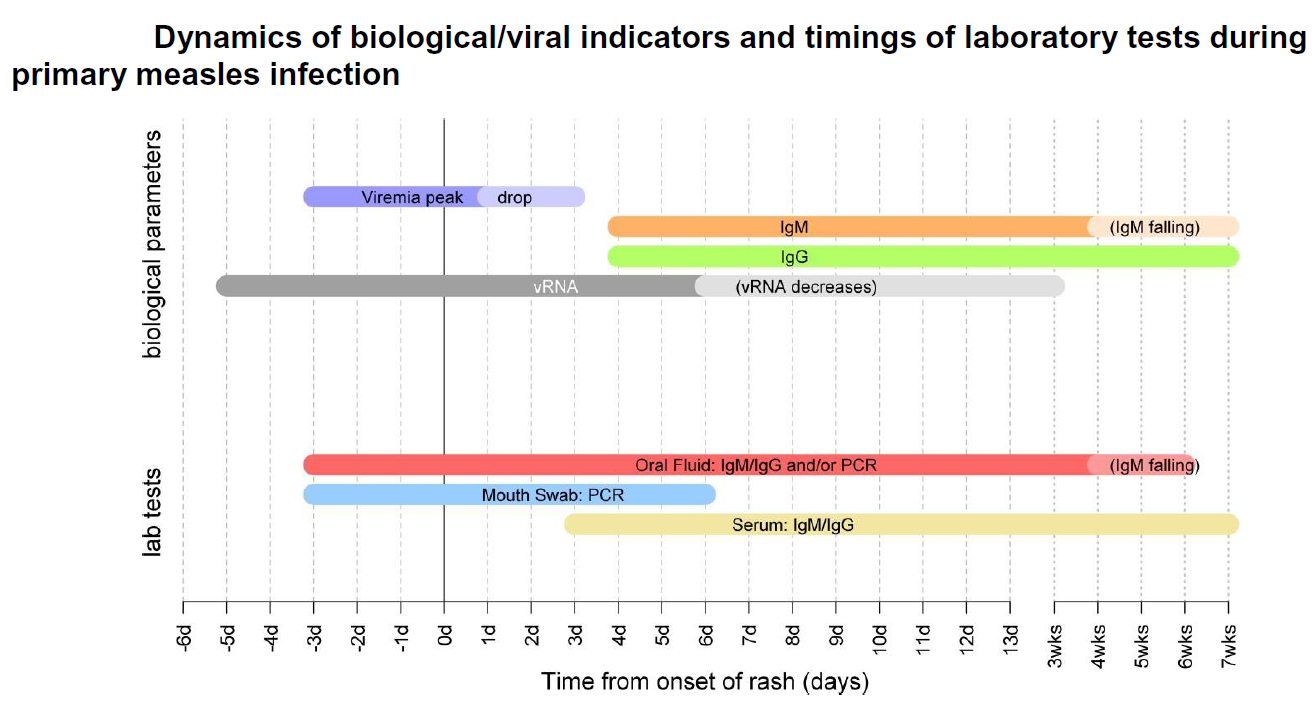
Diagnosis should be confirmed by laboratory testing in suspected cases (1). The following non-invasive methods can be used:
- salivary swab for measles specific IgM taken within six weeks of onset or
- serum sample for measles specific IgM taken within six weeks of onset or
- RNA detection in salivary swabs or other samples (1)
In Detail:
Measles is a single-stranded RNA virus (genus Morbillivirus, family paramyxoviridae)
- are 24 described genotypes, many of which have been eliminated as part of the global control of measles. Less than 10 genotypes are currently found globally, the distribution of which varies across geographic areas
- genotyping on confirmed samples is an integral part of laboratory surveillance for measles, to identify imported cases and monitor progress towards elimination
- oral fluid (OF) is the optimal sample for measles surveillance
- these samples are minimally invasive and are more acceptable than serum for confirming cases in infants and children. Importantly, OF can be tested for IgM, IgG and measles RNA, and can therefore:
- i) reliably exclude measles diagnosis, as well as confirm it;
- ii) indicate whether the case is primary or breakthrough measles (reinfection);
- and iii) genotype confirmed cases.
- these samples are minimally invasive and are more acceptable than serum for confirming cases in infants and children. Importantly, OF can be tested for IgM, IgG and measles RNA, and can therefore:
Oral fluid
- oral fluid (OF) is the optimal sample for measles surveillance and should be taken from all suspected cases regardless of any other samples that may have already been taken, including when other laboratory methods have not confirmed measles
- OF can be tested for both measles IgM/IgG using specific enzyme immunoassays (EIA), and viral RNA using specifically designed assays. Testing for IgM on OF is more sensitive and more specific than serum, particularly in the first few days after the rash, as IgM antibodies are positive in >50% of samples on day one of the rash, and in over 90% by day 3 of the rash .For oral fluid samples taken within 7 days of onset of disease, PCR analysis for RNA detection is also performed (2)
- OF can be tested for measles IgG, and although measles IgG avidity is not done on OF samples, the relative level of measles IgG can be used to predict whether the case is a primary or re-infection with measles
- measles viral RNA can be detected from before the onset of the rash and for at least 2 weeks after the onset of symptoms. Genotyping for molecular epidemiology can be performed on PCR positive samples, which allows the characterisation of the virus into one of the 24 known genotypes, and help identify clusters and imported cases
- measles genotyping also allows the distinction between wild-type virus and vaccine in those developing a measles-like rash following vaccination
- it is important to note that oral fluid samples cannot be used to assess the immune status of vulnerable contacts and serum should be used instead
Serum
- serum samples can be used for IgM/IgG detection through enzyme immunoassays (EIA)
- serum is the most appropriate sample to assess the immune status of contacts
- serum samples may still be IgM negative within 3 days of onset of rash - this may be longer for IgM assays used in some laboratories - the timing of the sample in relation to rash onset is therefore essential to properly interpret results
- serum can be used to confirm breakthrough measles (reinfection) by detection of high avidity measles IgG
- serum is not suitable for PCR detection and viral typing
- serum cannot be used to distinguish wild-type measles from vaccine-derived measles following recent vaccination
Mouth swabs
- mouth swabs can be used for PCR if collected within 6 days of the onset of rash. A negative PCR result does not exclude a diagnosis of measles
- mouth swabs can be used to distinguish between wild-type virus and vaccine in someone who has recently been vaccinated
- mouth swabs cannot be used to distinguish between a primary infection and a breakthrough measles (reinfection)
Throat swabs/Nasopharyngeal Aspirate/Urine/EDTA blood
- such samples can be used for PCR if collected within 6 days of the onset of rash
- such samples are less suitable than the others mentioned and generally not advisable for measles testing (2)
Reference:
- (1) Asaria P, MacMahon E. Measles in the United Kingdom: can we eradicate it by 2010? BMJ. 2006;333(7574):890–895
- (2) Public Health England (November 2019). National measles guidelines.
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.