Antibiotic treatment in community acquired pneumonia (CAP)
- assess severity in adults based on clinical judgement guided by mortality risk score (CRB65 or CURB65):
- low severity – CRB65 0 or CURB65 0 or 1
- moderate severity – CRB65 1 or 2 or CURB65 2
- high severity – CRB65 3 or 4 or CURB65 3 to 5
- 1 point for each parameter: confusion, (urea >7 mmol/l), respiratory rate ≥30/min, low systolic (<90 mm Hg) or diastolic (≤60 mm Hg) blood pressure, age ≥ 65
- assess severity in children based on clinical judgement
- offer an antibiotic. Start treatment as soon as possible after diagnosis, within 4 hours (within 1 hour if sepsis suspected and person meets any high risk criteria)
- when choosing an antibiotic, take account of severity, risk of complications, local antimicrobial resistance and surveillance data, recent antibiotic use and microbiological results
NICE has outlined the principles of management of community acquired pneumonia (1)
Notes:
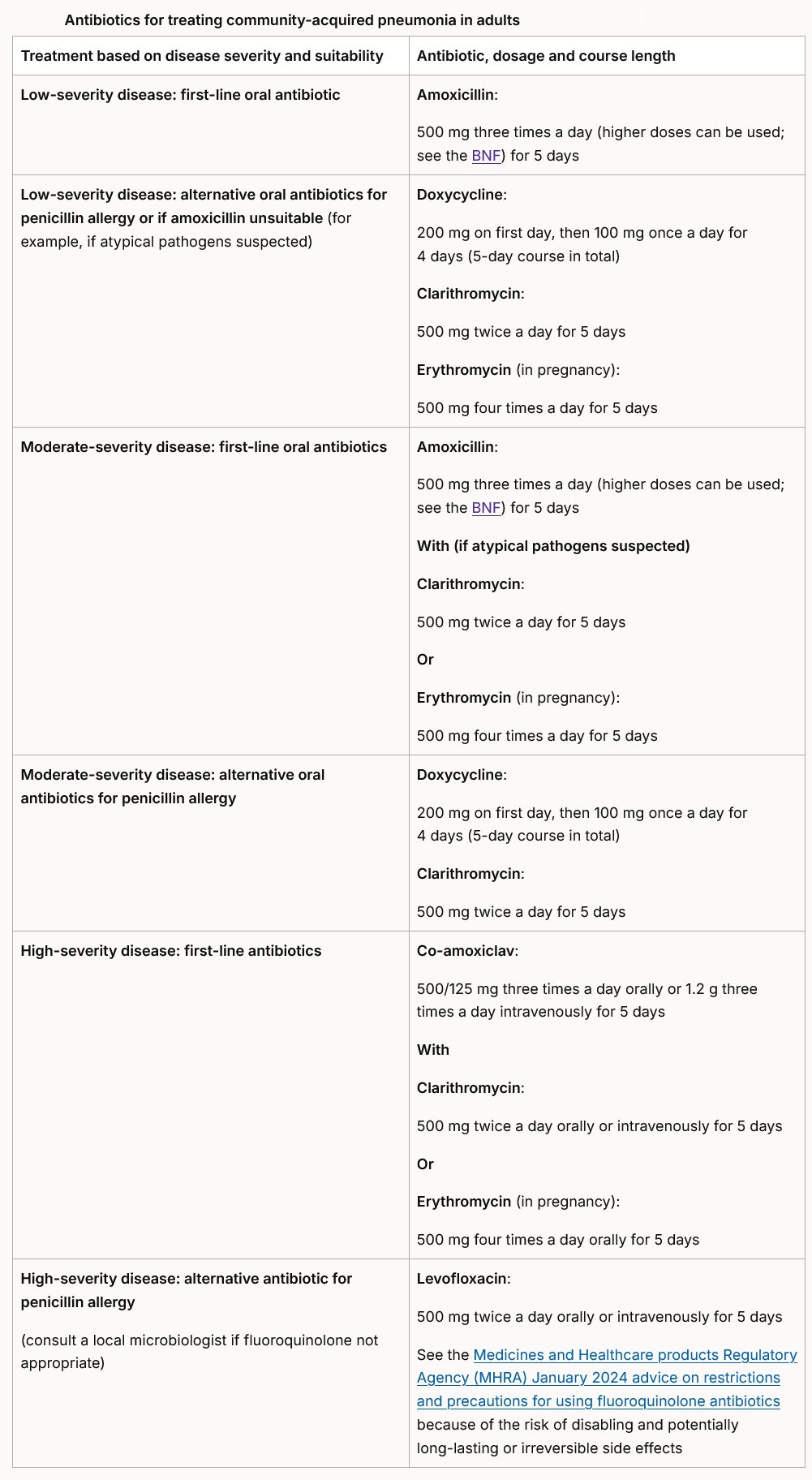
- for erythromycin: erythromycin is preferred if a macrolide is needed in pregnancy, for example, if there is true penicillin allergy and the benefits of antibiotic treatment outweigh the harms
- see the Medicines and Healthcare products Regulatory Agency (MHRA) Public Assessment Report on the safety of macrolide antibiotics in pregnancy
- for amoxicillin with clarithromycin or erythromycin if atypical pathogens suspected: mycoplasma pneumoniae infection occurs in outbreaks approximately every 4 years. If used as first-choice oral antibiotics if moderate severity, consider adding a macrolide to amoxicillin if atypical pathogens suspected. Review when microbiological results available
- for levofloxacin, see the MHRA January 2024 advice on restrictions and precautions for using fluoroquinolone antibiotics because of the risk of disabling and potentially long-lasting or irreversible side effects
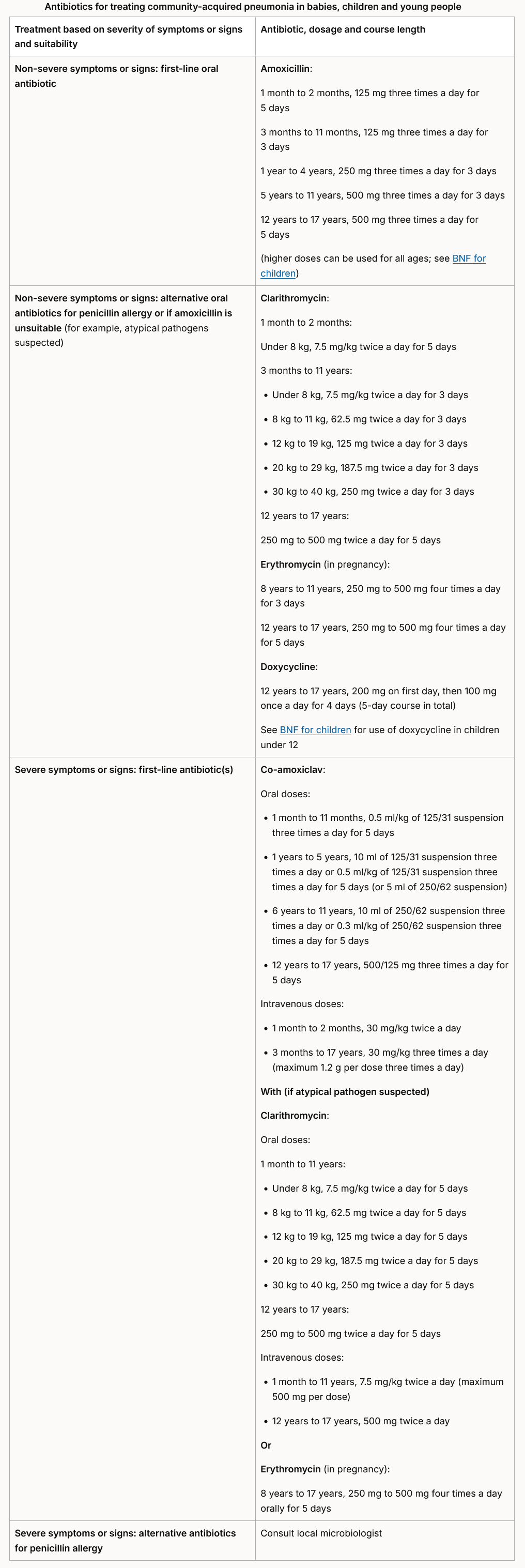
Antibiotics for children with community acquired pneumonia (1):
- offer a 3‑day course of antibiotics for babies and children aged 3 months (corrected gestational age) to 11 years with non-severe community-acquired pneumonia without complications or underlying disease
- consider extending use of antibiotics beyond 3 days for babies and children aged 3 months (corrected gestational age) to 11 years if they are not clinically stable, for example, if they are in respiratory distress or their oxygen saturation levels have not improved as expected
- for all children and young people with community-acquired pneumonia, stop antibiotic treatment after 5 days unless microbiological results suggest a longer course is needed or the child or young person is not clinically stable
Reference:
Related pages
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.