Prognosis of CLL
In patients with CLL:
- one third will not require treatment and have a long survival
- one third will have an initial indolent phase followed by disease progression
- remaining third presents with aggressive disease and will need immediate treatment (1)
The median survival of patients with CLL at diagnosis differs between 1 and >10 years (2,3).
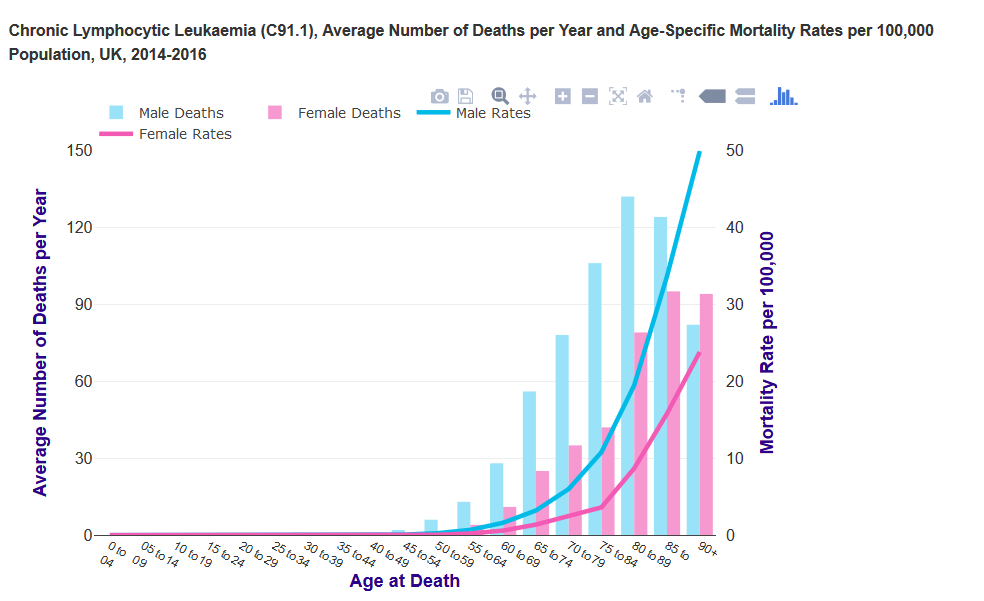
UK data (2):
- chronic lymphocytic leukaemia mortality is strongly related to age, with the highest mortality rates being in older people
- in the UK in 2014-2016, on average each year around three-quarters (74%) of deaths were in people aged 75 and over
- largely reflects higher incidence and lower survival for chronic lymphocytic leukaemia in older people
- age-specific mortality rates rise steeply from around age 60-64. The highest rates are in the 90+ age group for males and females. Mortality rates are significantly higher in males than females in a number of (mainly older) age groups. The gap is widest at age 50 to 54, when the age-specific mortality rate is 5.8 times higher in males than females
Although Rai and Binet staging systems are used to predict the prognosis in CLL, neither of the two systems can
- identify patients with indolent or progressive disease
- predict the response to treatment (4).
In addition to clinical staging, the following traditional factors have some value but also have important drawbacks (1)
- short lymphocyte doubling time
- diffuse bone marrow infiltration
- high serum levels of b2-microglobulin
- high serum levels of soluble CD23 (4)
Therefore newer prognostic markers have been proposed to identify risk of disease progression:
- immunoglobulin variable region heavy chain gene (IgVH) mutation
- in IgVH mutation - median survival is more than 20 to 25 years
- in unmutated IgVH - the survival is 8 to 10 years
- chromosomal abnormalities by fluorescent in situ hybridization (FISH)
- with this method over 80% of chromosomal abnormalities in the CLL patients has been identified
- deletion 13q -
- the commonest cytogenetic abnormality (55%)
- is associated with a favourable prognosis and longest survival
- deletion of 11q
- found in 18% of the patients
- is associated with development of extensive lymphadenopathy and shorter survival (79 months)
- deletion 17p13 -
- has the poorest prognosis
- is linked to shorter treatment free intervals, shorter survival (32 months), and resistance to therapy
- ZAP-70 (an intracellular protein tyrosine kinase, which plays a critical role in T-cell receptor signalling)
- in positive ZAP-70 - median survival is 6-10 years
- in negative ZAP-70 - survival was more favourable (>15 years) (4)
- CD38 immunophenotype
- CD38 positivity (>30%) is associated with a worse prognosis (5)
- it is important to note that the optimum cut off value is uncertain (1)
Note:
- the presence of poor prognostic factors should not be used to start treatment earlier in asymptomatic patients (4)
Reference:
- 1. Dighiero G, Hamblin TJ. Chronic lymphocytic leukaemia. Lancet. 2008;371(9617):1017-29.
- 2. CRUK.Chronic lymphocytic leukaemia (CLL) mortality statistics (Accessed 28/5/19)
- 3. Eichhorst B et al. Chronic lymphocytic leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010;21 Suppl 5:v162-4
- 4. Pinilla-Ibarz J, McQuary A. Chronic lymphocytic leukemia: putting new treatment options into perspective. Cancer Control. 2010;17(2 Suppl):4-15
- 5. National Cancer Institute at the National Institutes of Health. Chronic Lymphocytic Leukemia Treatment. Stage information for chronic lymphocytic leukemia
Related pages
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.